DKA ddx
- related: DKA
DKA ddx:
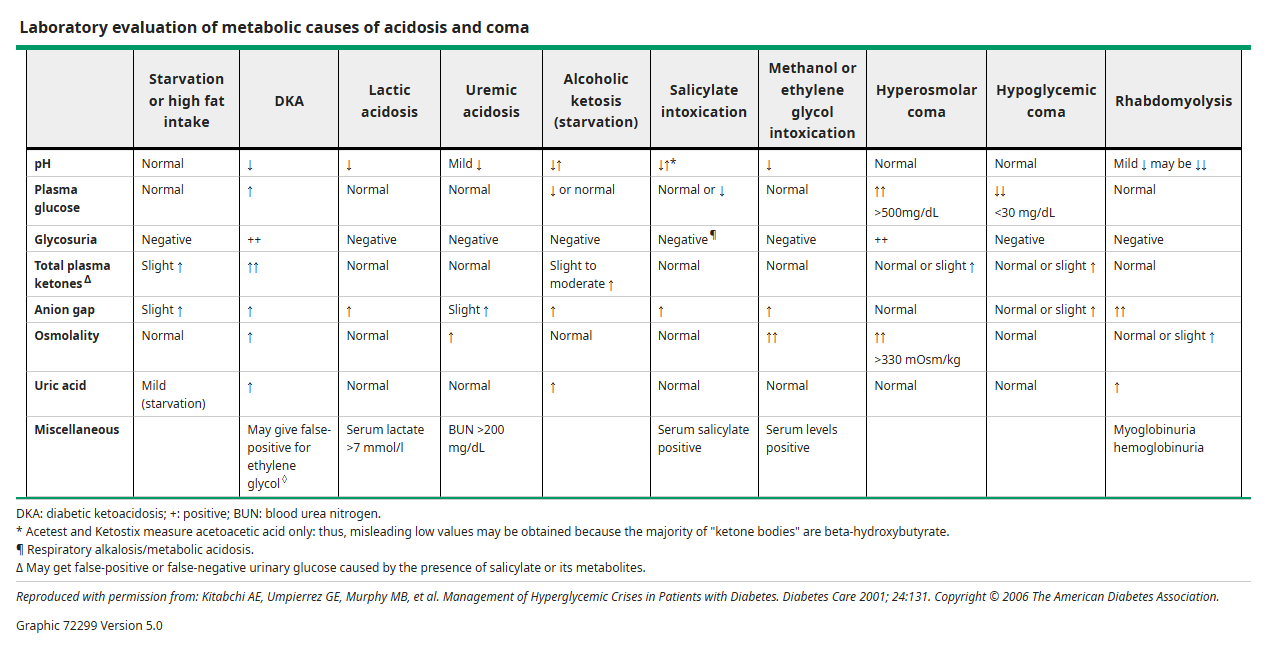
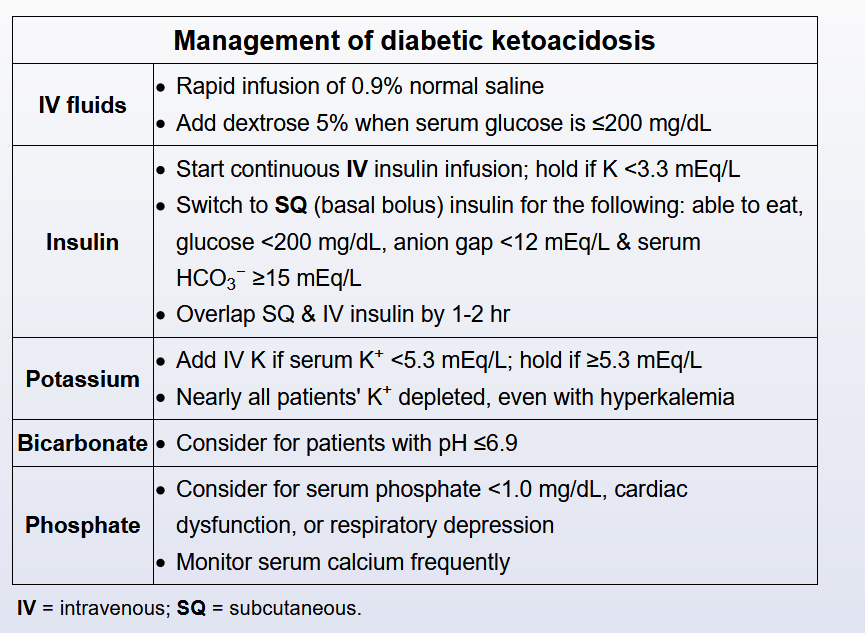
Alcoholic and fasting ketoacidosis — Alcoholic ketoacidosis (AKA) and starvation ketosis are other causes of ketoacidosis. Low-carbohydrate diets can also precipitate ketoacidosis. Metabolic acidosis can be relatively severe in patients with AKA. However, when ketoacidosis develops as a result of starvation, it is usually relatively mild. Ketoacid levels with prolonged fasting rarely exceed 8 to 10 mEq/L, and the serum bicarbonate concentration is typically greater than 17 mEq/L. More severe ketoacidosis may develop with prolonged fasting in children and pregnant women.
Ketoacidosis without hyperglycemia in a patient with chronic alcoholism is virtually diagnostic of AKA. Modest elevations in serum glucose in patients with alcoholic ketoacidosis may reflect underlying unrecognized diabetes or a catecholamine-mediated stress response. Measurement of glycated hemoglobin (A1C) can confirm chronic hyperglycemia.
Anion gap acidosis — Diabetic ketoacidosis (DKA) must be distinguished from other causes of high anion gap metabolic acidosis including lactic acidosis (which can rarely be associated with, or generated by, metformin, particularly in patients with impaired renal function); aspirin or acetaminophen toxicity and poisoning with methanol, ethylene glycol, and propylene glycol; D-lactic acidosis; and advanced chronic kidney disease. Although none of these disorders cause ketoacidosis, several different types of acidosis may coexist, especially lactic acid and ketoacidosis.
Metabolic encephalopathy — Toxic metabolic encephalopathy is usually a consequence of systemic illness, and its causes are diverse. In patients with diabetes, both severe hypoglycemia and severe hyperglycemia can result in coma. Measurement of fingerstick (capillary) or plasma glucose may be diagnostic.